Depending on the patient and various other factors, it is sometimes appropriate to undertake coronary angiography. This is done to visualize the coronary vessels. Thus, when valve surgery is undertaken, any co-existing narrowings in these vessels can be tackled at the same time.
Cardiac surgery is usually done “on bypass”. This means that during the operation, an artificial circulation is applied that “bypasses” the heart to maintain the circulation. More recently, less invasive surgery can be undertaken avoiding thoracotomy, and this is called “minimally invasive” cardiac surgery. Instead of splitting the breast bone, which is associated with a more prolonged postoperative recovery time, this technique uses smaller incisions in the right chest, and recovery times are quicker. However, not all patients are suitable due to technical issues, but the feasibility can be discussed with the surgeon.
Actual valve surgery may involve a valve being repaired (usually this applies to the mitral valve). Otherwise, a metal valve (metal prosthesis) can be used to replace the leaky or narrow. The advantage of this type of valve is that they tend to last a very long time, and may never need to be replaced. So, this is more likely in younger patients. The disadvantage of metal valves, are that they require anticoagulation with warfarin to prevent clots building up. Alternatively, some form of biological valve may be used instead. These have the advantage of not requiring long term anticoagulation, but have the disadvantage of not lasting as long as metal ones. Thus, they may be more applicable in older patients or in those who have bleeding problems. In any cardiac surgical consultation, all the above factors would be evaluated.
Post operatively, patients are in hospital for between 5-10 days. Younger fitter patients tend to have a shorter length of stay, and older patients or with other existing medical conditions, have a longer stay.
Early complications include some renal disturbances, chest infections and occasionally neurological disturbances. A lot of attention is spent prior to surgery in treating any risks for these conditions to avoid complications. A sore chest after the operation is the most likely side effect, but good pain relief and breathing techniques will minimise this.
Postoperatively it is amazing how quickly patients are back on their feet. Initially after the operation, the patient is first ex-tubated from the breathing machine. Within 48 hours, most forms of plastic drains are removed, the patient is mobilized and physiotherapy started. Recovery is generally quicker and with fitter and slimmer patients. In any patient being considered for cardiac surgery, it is an opportunity to try and get healthier beforehand.
Cardiac risk factors:
- Smokng,
- Hypertension,
- Diabetes,
- Family history/other genetic factors
- Miscellaneous causes.
|


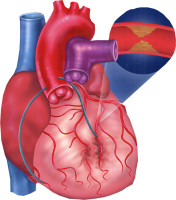 This is used to treat either patients requiring grafts to bypass narrowings in coronary arteries, or valve surgery, or both. Please read the section on heart valves first. If surgery is considered as the definitive treatment for valvular disease, certain points need to be borne in mind. First, the timing of surgery is crucial. Patients may have their valvular conditions monitored by echocardiography for years before surgery is indicated. But certainly, any development of symptoms such as breathlessness or dizziness etc. would bring surgery forward. Certainly if symptoms were to develop before the next review date, then an earlier appointment should be expedited. For arterial grafts, please see the section on “Coronary Artery Disease” first.
This is used to treat either patients requiring grafts to bypass narrowings in coronary arteries, or valve surgery, or both. Please read the section on heart valves first. If surgery is considered as the definitive treatment for valvular disease, certain points need to be borne in mind. First, the timing of surgery is crucial. Patients may have their valvular conditions monitored by echocardiography for years before surgery is indicated. But certainly, any development of symptoms such as breathlessness or dizziness etc. would bring surgery forward. Certainly if symptoms were to develop before the next review date, then an earlier appointment should be expedited. For arterial grafts, please see the section on “Coronary Artery Disease” first.