Treatment of atrial fibrillation will depend on the particular type. For isolated episodes (called paroxysmal AF) sometimes no treatment is warranted. For more bothersome attacks, regular medication is tried, usually with a beta-blocker in the first instance.
Radiofrequency ablation can be used for more curative action if medication is ineffective or causes side effects. For persisting atrial fibrillation where the disturbance is sustained, an electric shock (quite painless with very brief general anaesthetic) can normalise the heart rhythm. This is referred to as electrical cardioversion (see below). Once again, for recurring episodes of persisting atrial fibrillation, radiofrequency ablation should be considered. Some types of atrial fibrillation are longstanding or might be resistant to electrical shock. In some of these cases, it might be deemed as unnecessary or impossible to convert the rhythm back. This is so called “permanent atrial fibrillation”, and the mainstay of treatment is to control the heart rate instead,usually with beta-blockers or digoxin.
Risk of Stroke in AF:
Despite causing symptoms which may disruptive, AF is generally a benign condition. However, the main concern is the associated risk of stroke. This occurs when the irregular rhythm results in relative stagnation of blood flow in certain parts of the left atrium, causing clot to build up. If a small bit of clot dislodges, it can fly off into the brain. This is worrying and the potential risk of it occurring needs to be assessed. Where the risk of stroke is considered significant, anticoagulation should be considered. Aspirin is no longer considered effective to prevent the risk of stroke. Traditionally, warfarin has been used to thin the blood. It still has its place in modern practice (especially in patients with heart valve replacements). However, the fact that it requires regular monitoring with blood testing (INR checks) may prove inconvenient for the elderly who may be less mobile, or the younger patients who are working. Adequate control is affected by dietary fluctuations (especially green vegetables) and alcohol, and there may be significant interactions with other medication. As a result, for many patients, a class of drugs called NOACS (novel oral anticoagulants) are being used. Examples include: Edoxaban, Apixaban, Rivaroxaban and Dabigatran. They do not require blood tests to monitor effectiveness and have far less interactions with lifestyle and other medications.
The benefits and risks of anticoagulation always need to be considered. A scoring system called CHADS-VASC is used to identify who would benefit most from the NOACS. In short, increasing age, the presence of known heart disease such as heart failure or coronary artery disease, diabetes and hypertension are associated with the risk of stroke and most likely to benefit. The main risk is that of bleeding, which can be assessed by another scoring system called the HASBLED Score. These scoring systems will help decide who would benefit from the medication and whether they are safe. Over time however, in the elderly, eventually the risks of bleeding may exceed the benefits.
Electrical Cardioversion:
This is the procedure to restore normal heart rhythm by electrically jolting the heart. Patients are prepared in the following way: The blood is thinned with warfarin for at least 4 weeks to dissolve any potential clots that would be dislodged by the electric shock. In some cases, the heart rhythm is stabilized electrically with a drug such as amiodarone for about three weeks. In this way when the electric shock is delivered there is a maximum chance of restoring a normal rhythm. For the actual procedure, the patient is fasted for 6 hours. The patient is very briefly aneasthetized and an electric shock delivered. Provided the patients are well selected, the overall success rate is about 80%. After the shock, the patient wakes up and can go home after about 4 hours. It is important that the patient remains on the existing medication for at least three weeks to prevent the risk of stroke, and to maximise the chance of success.
If necessary, cardioversion can be attempted for relapses back in to AF several times. Cardioversions are less successful when the left atrium is very enlarged, or there are signs of infection or the potassium is low.
Atrial Flutter:
This is a more regularised form of atrial fibrillation that conforms to a more defined circuit. It is sometimes more difficult to pick up clinically as the pulse on examination often feels regular. The treatment principles are fairly similar to that of fibrillation.
|


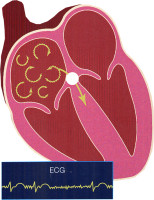 Atrial fibrillation is another type of SVT where the abnormal electrical pathway is totally erratic. It is a very common arrhythmia, that becomes more prevalent with increasing age. It may be incidentally picked up on a routine ECG, where the person is asymptomatic, or most commonly, the person may experience palpitations. Others however, may experience fatigue, dizziness or breathlessness on exertion.
Atrial fibrillation is another type of SVT where the abnormal electrical pathway is totally erratic. It is a very common arrhythmia, that becomes more prevalent with increasing age. It may be incidentally picked up on a routine ECG, where the person is asymptomatic, or most commonly, the person may experience palpitations. Others however, may experience fatigue, dizziness or breathlessness on exertion.